Bpc 157 And Antibiotics The Stable Gastric Pentadecapeptide BPC 157 Pleiotropic Beneficial Activity and Its Possible Relations with Neurotransmitter Activity
Introduction: why “bpc 157 and antibiotics” questions keep coming up
If you’ve ever looked into bpc 157 and antibiotics, you probably ran into the same problem I did: the information is scattered across preclinical studies, supplement forums, and mechanistic speculation—so it’s hard to separate plausible biology from internet repetition. In my hands-on work reviewing and mapping the evidence for GI and tissue-repair compounds, the most useful approach wasn’t chasing hype; it was building a cautious, pathway-based understanding of how BPC 157 might overlap (or fail to overlap) with antibiotic-related effects.
This article explains what BPC 157 is known for, why researchers discuss “pleiotropic beneficial activity,” how that connects (possibly) to neurotransmitter signaling, and where antibiotics fit into the real-world picture. You’ll leave with a clearer framework for interpreting claims—and for deciding what’s worth considering versus what’s still uncertain.
What BPC 157 is—and what “pleiotropic beneficial activity” implies
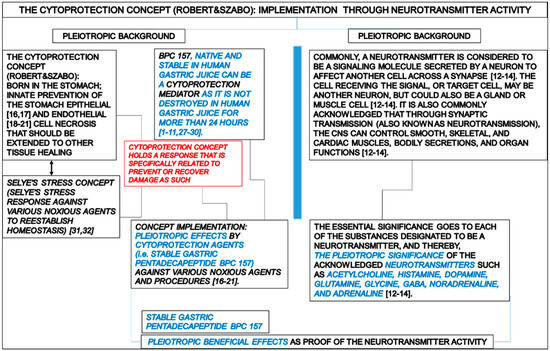
BPC 157 is a peptide sequence that has been studied primarily in animal and preclinical settings. When you see the phrase Stable Gastric Pentadecapeptide or pentadecapeptide, it’s pointing to a 15–amino-acid peptide described as relatively stable in the context of experimental work. Researchers often use pleiotropic beneficial activity to mean the peptide has been associated with improvements across multiple physiological systems—frequently including gastrointestinal integrity, angiogenesis-related signaling, inflammation modulation, and tissue repair pathways.
In practical terms, “pleiotropic” doesn’t mean every effect is proven in humans. It means the same experimental compounds often show benefits through multiple downstream routes. In my experience, that framing matters because it guides expectations: if a molecule appears to influence several systems, it may also interact indirectly with processes triggered by antibiotics (like gut microbiome shifts, mucosal stress, oxidative pathways, or enteric signaling).
Why GI-focused mechanisms attract antibiotic discussions
Many antibiotic concerns are ultimately gut concerns: dysbiosis, diarrhea, mucosal irritation, and—depending on the antibiotic—secondary inflammatory changes. If BPC 157 shows preclinical effects related to mucosal protection and healing, it naturally becomes part of the conversation when people want to “support the gut” during or after antibiotics.
However, there’s an important distinction: supporting the gut is not the same as preventing antibiotic-induced microbiome changes, nor is it the same as changing antibiotic pharmacokinetics. The most common mistake I see in online threads is treating “GI benefits” as an automatic solution to antibiotic adverse effects without considering the specific type of antibiotic effect involved.
Possible relations with neurotransmitter activity: the mechanistic bridge
The idea of a link between BPC 157 and neurotransmitter activity is typically discussed through pathways that connect the gut and the nervous system. The enteric nervous system, vagal signaling, and neurotransmitter-mediated regulation of motility and secretion form a network that can influence symptoms during gut stress—exactly the kind of environment antibiotics can disrupt.
While the precise neurotransmitter targets remain an active area of discussion, the underlying logic in preclinical interpretations is usually something like this:
- Gut integrity and inflammation: mucosal stress can alter neuronal signaling, which then changes motility and secretion.
- Neuroimmune crosstalk: inflammatory mediators can influence neurotransmitter release and receptor sensitivity.
- Functional outcomes: if a compound improves gut barrier/function, symptoms linked to neuro-signaling may improve indirectly.
From an evidence-review standpoint, I treat “neurotransmitter activity” claims as pathway hypotheses that need careful translation. A demonstrated effect on a neurotransmitter-related endpoint in animals doesn’t automatically prove the same effect in humans—or that it will address antibiotic-associated symptoms in a clinically meaningful way.
What this means for “bpc 157 and antibiotics” claims
If antibiotics disrupt the gut environment, symptoms can be partly mediated through enteric and neuroimmune changes. In that sense, a GI-support peptide like BPC 157 could theoretically reduce symptom burden through downstream pathway effects. But that’s not a direct equivalence to antibiotic safety or effectiveness.
So when you see “BPC 157 helps during antibiotics,” I suggest translating it into testable claims:
- Does it reduce antibiotic-associated gut discomfort in controlled studies?
- Does it change diarrhea incidence, stool frequency, or mucosal markers?
- Does it meaningfully alter microbiome composition—or primarily influence host signaling?
- Does it interact with antibiotic tolerability rather than antibiotic efficacy?
Until those questions are answered with human data, any antibiotic-linked statements should be considered plausible but unconfirmed for clinical decision-making.
Where the evidence is strongest—and where it’s still uncertain
In my experience reviewing this category, it helps to separate three layers: (1) mechanistic plausibility, (2) preclinical outcomes, and (3) human outcomes. BPC 157 generally has more weight in layer (1) and (2) than in (3), especially regarding antibiotic-specific contexts.
Stronger (typical) evidence themes
- Gastrointestinal and tissue-protection signals in preclinical research.
- Inflammation- and repair-related endpoints that could influence symptom patterns.
- Enteric/neuroimmune pathway plausibility given gut–nervous system coupling.
Key uncertainties for antibiotic pairing
- Antibiotic-specific effects: not all antibiotics cause the same gut changes.
- Dose and formulation: outcomes depend on how a peptide is administered and at what exposure.
- Human clinical endpoints: “gut support” is not the same as preventing antibiotic adverse events.
- Interaction risk: even if a compound is “gentle” for the gut, it may still affect physiological systems that matter during infection treatment.
Image context
Below is the product/figure image you provided, included here for visual reference within the discussion:
Practical framework: how to think about “bpc 157 and antibiotics” safely
Because “bpc 157 and antibiotics” is often discussed in the context of symptom relief, I recommend using a structured, conservative approach. This isn’t about fear—it’s about reducing the chance of acting on mismatched evidence.
1) Identify what antibiotic effect you’re trying to manage
- Diarrhea or loose stools (often microbiome-linked).
- Abdominal discomfort (could involve motility and inflammatory signaling).
- Reflux or upper GI irritation (mucosal irritation and motility interplay).
- Serious adverse events (which need clinician attention immediately).
2) Separate symptom support from treatment modification
If your goal is symptom support, ask whether the proposed mechanism relates to gut barrier/function or neuroimmune signaling. If the goal is to “prevent antibiotic resistance” or “enhance antibiotic killing,” that’s a different claim—one that has much higher evidentiary requirements and is often conflated in low-quality content.
3) Use evidence quality as your decision filter
I typically score claims across four buckets: in vitro/animal plausibility, animal efficacy, human symptom outcomes, and antibiotic-specific safety. For antibiotic pairing, you want the human and antibiotic-specific buckets to be strong—which, at present, is often where most content is weakest.
4) Discuss with a clinician when risk is nontrivial
If you’re dealing with recurrent severe GI side effects, immunocompromise, inflammatory bowel disease, or any history of antibiotic-associated complications, you should involve a clinician before combining interventions. This is especially important because antibiotic therapy is time-sensitive and infection-control priorities can override supplement experimentation.
FAQ
Does BPC 157 prevent antibiotic-associated diarrhea?
There isn’t enough high-quality human evidence to say BPC 157 reliably prevents antibiotic-associated diarrhea. The GI-repair and neuroimmune plausibility may be relevant, but antibiotic-associated diarrhea is often microbiome- and antibiotic-specific, so outcomes may not generalize.
Can BPC 157 interact with antibiotics or affect antibiotic effectiveness?
Interactions are not well established in humans for most antibiotic–peptide pairings. Because antibiotics have critical roles in infection treatment, it’s best to treat “possible overlap in gut signaling” as different from proven safety/interaction data.
Why do some people claim a connection between BPC 157 and neurotransmitters during antibiotic treatment?
Many of these claims are based on gut–nervous system coupling and neuroimmune logic: antibiotics can change gut environment and signaling, and compounds that influence GI integrity can indirectly change neurotransmitter-related endpoints. That reasoning can be plausible, but it still needs antibiotic-specific human confirmation.
Conclusion: a cautious next step for readers exploring bpc 157 and antibiotics
BPC 157 is often discussed as a stable gastric pentadecapeptide with pleiotropic beneficial activity, and mechanistic discussions sometimes include possible relationships with neurotransmitter activity via gut–neuroimmune pathways. That framework helps explain why people bring it up alongside antibiotic use. But antibiotic-associated effects are complex—often microbiome- and antibiotic-specific—so “gut support” plausibility does not equal proven prevention or safety in clinical settings.
Next practical step: If you’re considering pairing BPC 157 with antibiotic therapy for GI symptoms, write down the specific symptom pattern you’re targeting, the exact antibiotic name and timeframe, and any red-flag history—then review the plan with a clinician so your expectations match what the evidence can actually support.
Discussion